What Care Home Software Needs to Do
Running a care home means managing a continuous flow of information. Good care management software connects all of it: digital social care records that update in real time, care planning software that adapts as needs change, medication rounds that need accurate recording. Staff rotas shift. Families want updates. CQC wants evidence. Every piece connects to every other piece, and the consequences of getting it wrong are serious.
At minimum, care home software needs to handle:
- Digital care plans (care planning software) with daily notes, observations, and risk assessments that update in real time
- Electronic medication administration records (eMAR) with alerts for missed or late doses
- Incident and accident reporting with audit trails for CQC inspections
- Staff rota management with shift patterns, availability tracking, and compliance with staffing ratios
- Family communication so relatives can see how their family member is doing without phoning the home
- CQC compliance tools that generate the evidence inspectors ask for, not after the fact, but as part of the daily workflow
More advanced systems also cover occupancy and bed management, supplier and procurement tracking, financial reporting, and integration with pharmacy systems for automated medication ordering.
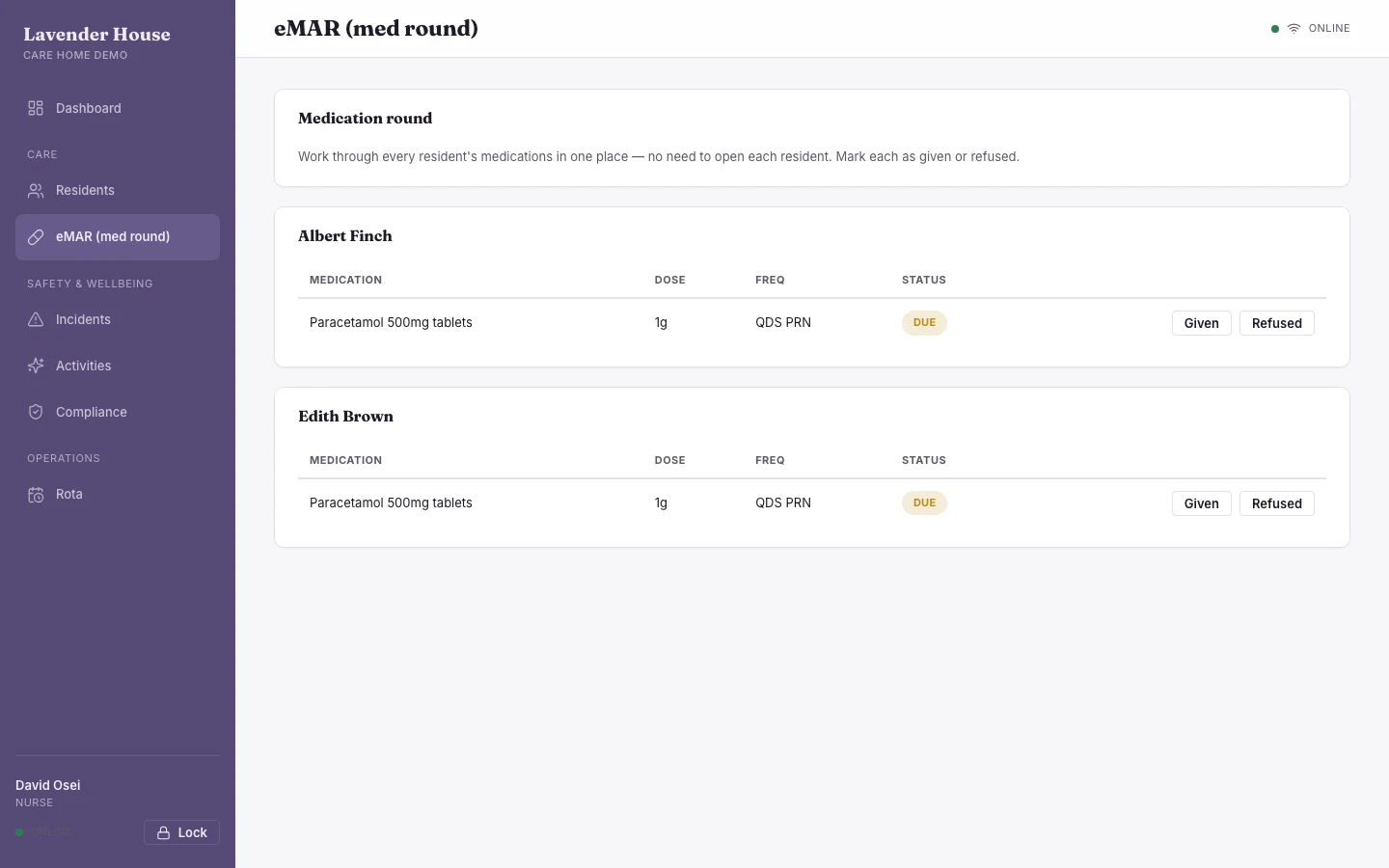
Inside the live care home software demo
A simple demo for care homes. Open it as a nurse and run a medication round on the eMAR, or as a family member and see the portal updates. It handles the core daily work:
- Digital care plans that update in real time and stay aligned with CQC requirements.
- eMAR medication rounds with full recording and alerts for the round.
- Staff rotas and handovers so shifts and notes pass cleanly between teams.
- Family portal for relatives to see selected updates without extra logins or calls.
- CQC-ready records and DSPT evidence built as you work, not as a separate job.
We build your system around your home and you own it outright. The build cost is upfront, but over two to three years you save significantly against subscription fees.
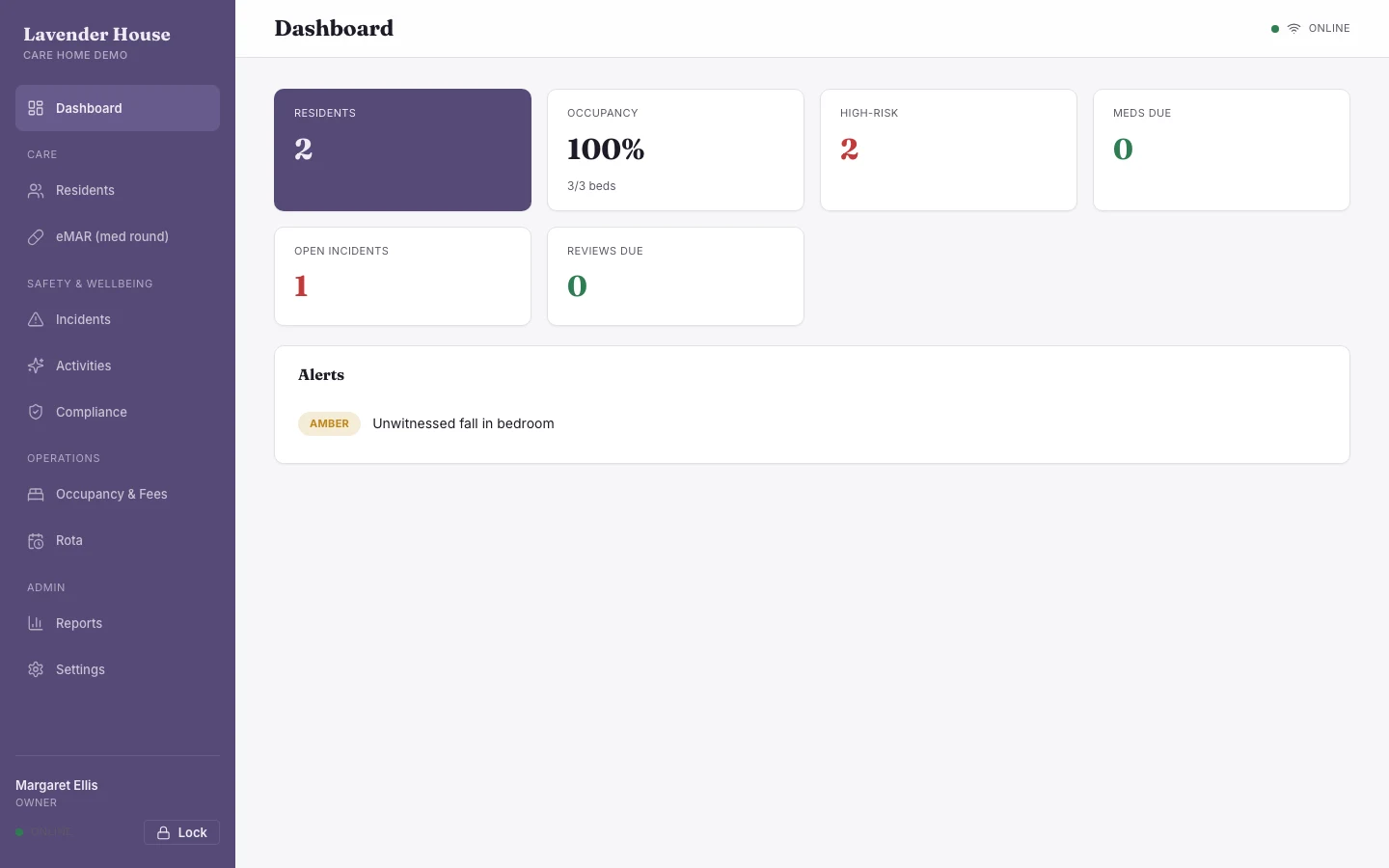
A simplified live demo. Choose a user to explore as, no login needed. Open full screen →
The Main Options in the UK Right Now
The UK care home software market is dominated by a handful of providers. Here is a look at what is available and what each one actually delivers.
| Provider | What They Offer | Pricing | Best For |
|---|---|---|---|
| Person Centred Software | The largest in the UK. Used by over 8,000 providers. Full digital care system: care planning, eMAR, wellbeing tracking, operations. Comprehensive but complex. | Not publicly disclosed. Subscription-based. Contact for quote. | Large care groups with dedicated IT support and budget for a premium system. |
| Birdie | Modern, well-designed platform focused on domiciliary and home care. Care management, scheduling, medication, finance. Strong mobile app. | From £200/month. Usage-based on care hours. Mandatory implementation package for 300+ care recipients. | Home care and domiciliary providers. Less suited to residential care homes. |
| CareDocs | Stand-alone care planning system. Digital care plans, eMAR, incident reporting. Lower cost, simpler to implement. Used widely by smaller residential providers. | Approximately £1.50 to £3 per resident per month, plus setup fees. | Smaller residential homes looking for a straightforward, affordable system. |
| Nourish | Care management with a focus on person-centred recording. Care plans, handovers, observations, family portal. Clean interface. | Subscription-based. Contact for quote. | Homes that want a modern interface with strong person-centred recording. |
| Log my Care | Free tier available for small providers. Digital care plans, observations, medication. Paid plans add more features. | Free for up to 25 service users. Paid plans from £2/service user/month. | Very small providers or those wanting to try digital records before committing. |
All of these are subscription-based. You pay monthly, indefinitely. The cost compounds over years. A home paying £200 per month for software spends £2,400 per year, £12,000 over five years, and still owns nothing. If you stop paying, you lose access to the system and, in many cases, your data.
Where Off-the-Shelf Falls Short
The platforms listed above are competent products. But they were all designed for a generalised version of a care home. Your home is not general.
Residential homes operate differently from nursing homes. Dementia care has different recording requirements from learning disability support. A home with 20 beds runs differently from one with 80. A home with an attached day centre has workflows that none of these platforms were built to handle.
What typically happens is this: you adopt the software, discover it does not quite fit how your home works, and you start building workarounds. A spreadsheet for the thing the software cannot track. A whiteboard for the rota because the software's rota feature does not match your shift patterns. A notebook for medication notes that do not fit the system's fields.
The other issue is control. When Person Centred Software or Birdie decides to change their interface, add features you did not ask for, or increase their prices, you have no say. You are renting their system on their terms. Your care records, the most sensitive data your business holds, live on their servers under their control.
Deep Dives
What a Bespoke Care Home System Looks Like
A bespoke system starts with your home. Not a template. Not a product demo. Your actual daily workflow, from handover to medication round to care plan review to family communication to CQC evidence generation.
We sit down with you and map exactly how your home operates. Then we build a system that matches it precisely. The result is software where every screen, every form, and every report reflects the way your staff actually work.
What we can build for care homes
Every system starts with your specific requirements. We design it around how your home actually operates, not around a fixed feature list. Here are examples of what your system could include:
- Care plans that match your recording style. Whether you use person-centred narrative notes, structured observations, or a combination, the system reflects your approach, not a vendor's template.
- Medication management built to your rounds. eMAR configured around your specific medication rounds, your PRN protocols, your controlled drugs procedures. Alerts and escalation paths that match your clinical governance structure.
- Staffing and rota management that fits your patterns. Your shift types, your bank staff arrangements, your ratio requirements. Not a generic rota tool that you have to force into shape.
- Family access on your terms. A portal where families see what you want them to see: daily updates, photos, care plan summaries. Controlled by you, not by a vendor's default privacy settings.
- CQC evidence built into the workflow. Every daily action your staff takes generates the evidence CQC asks for. No separate reporting step. No last-minute scramble before inspections.
- Analytics that answer your questions. Occupancy trends, staffing costs, incident patterns, medication adherence rates. The metrics that matter to your home, not the metrics a software vendor decided to include.
Speak to us about care home software · +44 7494 618 651 · Mon to Fri, 9am to 6pm
The Digital Social Care Records Landscape
The UK government's position is clear. The Department of Health and Social Care published its "What Good Looks Like" framework in 2023, setting out expectations for digital maturity across adult social care. The NHS England information standard (DAPB4102) defines the minimum data that CQC-registered providers should record digitally.
Four in five care providers have already adopted digital social care records. The direction is unambiguous. CQC inspectors increasingly expect to see digital systems during inspections, and providers still relying entirely on paper records face harder conversations about the quality of their evidence.
This is not a future trend. It is the present reality. If your home has not yet moved to digital records, or if you adopted a system that does not properly fit your needs, now is the time to address it.
What It Costs
ESRE builds care home systems for a one-off cost. No monthly subscription. No per-resident fees. No price increases. You pay once and you own the system.
Common subscription costs across the sector
Most care homes do not pay for one system. They pay for several, each covering a different part of the operation. For a 40-bed residential home, the monthly software spend across these tools often looks something like this.
| System | Typical Monthly Cost | Examples |
|---|---|---|
| Care planning and daily records | £200 to £400 | Person Centred Software, Nourish, Log my Care |
| eMAR (electronic medication) | £100 to £200 | Atlas eMAR, Medisafe, built-in module (extra cost) |
| Staff rostering and HR | £100 to £150 | PeoplePlanner, RotaCloud, Deputy |
| Family communication portal | £50 to £90 | Often an add-on to the care platform |
| Compliance and training tracking | £30 to £80 | Blue Stream Academy, Care Academy |
| Total monthly cost | £480 to £920 | |
| Five-year total | £28,800 to £55,200 |
None of these systems talk to each other properly. A medication change recorded in the eMAR does not update the care plan automatically. A rota change in the scheduling tool does not reflect in the compliance system. Staff enter the same information in multiple places. The "integrated" care home is actually five disconnected subscriptions held together by manual processes.
What a bespoke system costs
| System Scope | Typical One-Off Cost | Replaces |
|---|---|---|
| Core: care plans, eMAR, daily notes, CQC reporting | £8,000 to £15,000 | Care planning + eMAR subscriptions (£300-600/mo) |
| Full: above plus rostering, family portal, compliance, analytics | £15,000 to £30,000 | All five subscription categories above (£480-920/mo) |
| Multi-site: full system across 3 to 10 homes with central oversight | £25,000 to £60,000 | Per-home subscriptions multiplied across every location |
A 40-bed home paying £600 per month across its software stack spends £36,000 over five years and owns nothing at the end. A bespoke system at £20,000 pays for itself in under three years, replaces every subscription, and belongs to the home permanently. After year three, every month is pure savings.
Your Code, Your Control
Every system we build, the client owns all the code. There is no vendor lock-in. No proprietary platform you depend on. No API that gets deprecated when the vendor decides to change direction.
One data source, multiple applications
What we build is not one screen. It is a connected data architecture from which multiple applications emerge. A resident's information is entered once and appears wherever it is needed, in the right format for whoever is using it.
- A care recording interface for nurses and carers on the floor, optimised for quick entry during rounds
- A medication administration screen designed for the eMAR workflow, with barcode scanning and real-time recording
- A family portal where relatives see daily updates, photos, and care plan summaries without calling the home
- A manager dashboard showing occupancy, staffing ratios, compliance status, and incident trends at a glance
- CQC evidence exports that pull the data inspectors need into a format they can review quickly
All of these surfaces draw from the same data. A medication change recorded by a carer is immediately visible to the family, the manager, and the CQC export. No syncing. No re-entry. No "the system doesn't talk to the other system."
Building on top of what already exists
We train you and your team to evolve the system using AI. Since December 2025, AI tools have reached the maturity to work reliably alongside people for maintaining and extending systems. We set up your AI to understand your specific codebase, with failsafe environments, version control, and automated backups, so you can make changes yourself with confidence.
Because the data architecture already exists, adding new functionality is straightforward and inexpensive. Need a GP handover report that did not exist at launch? It can be built in days, not weeks, because all the data it needs is already in the system. Want to add a procurement module for supplies? It connects to the same resident and staff records. The initial build creates the foundation. Everything after that is incremental, and much of it can be done in-house with the tools we provide.
See examples of what we build across different sectors.
After five years, most care home software has cost you what bespoke costs once. And at the end of five years, you own nothing. Bespoke is a capital cost. It stays yours.
Rollback to the second, immutable records, encrypted family communications. Not an add-on module. It is in the architecture of every system we deploy.
Your residents' personal and clinical data on servers you control, in the UK. No SaaS vendor routing sensitive records through infrastructure you have no visibility of.
A core care management system covering residents, medication, staff, and compliance typically takes four to eight weeks from first conversation to live deployment.
Frequently Asked Questions
How long does it take to build?
A core care home system typically takes four to eight weeks from first conversation to live deployment. More complex systems with multiple modules and data migration from existing platforms take eight to twelve weeks.
Can you migrate data from our existing system?
Yes. We regularly import data from spreadsheets, legacy systems, and existing care management platforms. The goal is always a clean transition with no data loss.
What about ongoing support?
We are always available for support, changes, and enhancements. But because you own the code and we train your AI to understand it, you are not dependent on us for day-to-day changes. That is the point.
Where is the system hosted?
Your system is cloud-hosted on secure UK-based servers. Your data belongs to you. Every change is recorded in real time to a write-ahead log (WAL), so nothing is ever lost. You can also back up locally on a schedule for additional peace of mind.
What about CQC compliance?
CQC compliance is built into the daily workflow, not bolted on as a separate reporting module. Every note your staff writes, every medication they administer, every incident they record generates the audit trail that inspectors look for. When CQC arrives, the evidence is already there.
Can I try the care home software before committing?
Yes. There is a live care home demo you can open now, without a login. Open it as owner, nurse, senior carer, carer or family and use a working system. It is free to try; a production build is a one-off project that you own.